

Beyond STEMI in EMS
Why EMS Needs High-Risk ECG Notification on the Way to OMI

Every paramedic knows this call. Chest pain. Diaphoresis. A patient who does not look right. You acquire the 12-lead, stare at the tracing, and the monitor generates an ECG that quietly changes the rest of the patient’s day: Does Not Meet STEMI Criteria. Maybe there are broad T waves. Maybe there is reciprocal change that bothers you. But the system has trained everyone to listen for one word, and the word is not there.
So the patient goes in as chest pain. They wait for a room, wait for labs, and wait for a repeat ECG. All while an occluded coronary artery continues infarcting myocardium in real time.
That is the problem we must address.
The clinically important question is not whether the ECG meets millimeter criteria for ST elevation. The question is whether there is an acutely occluded coronary artery that would benefit from a more urgent reperfusion. STEMI is a useful signal when it is present; it is specific, familiar, and tied to a pathway that saves lives. But STEMI is one ECG expression of the disease. Occlusion myocardial infarction, or OMI, is the disease.
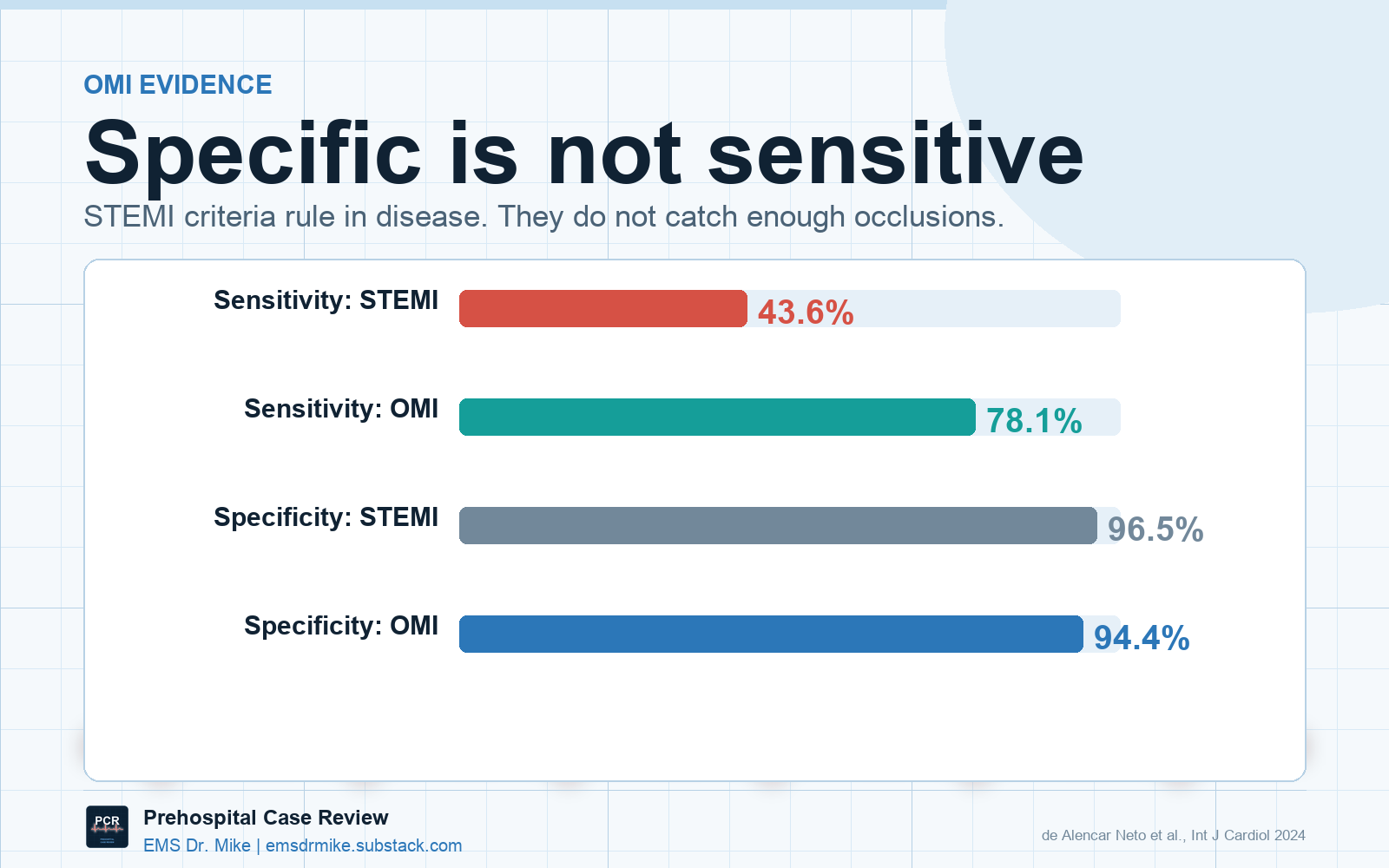
The data are no longer subtle. Across multiple cohorts, STEMI criteria miss a meaningful proportion of acute coronary occlusions. A 2024 systematic review found that ST elevation criteria had only 43.6% sensitivity for acute coronary occlusion, while an OMI approach improved sensitivity to 78.1% with only a modest specificity tradeoff [1]. Meyers and colleagues found that 40% of angiographically confirmed OMIs did not meet STEMI criteria [2], and expert OMI ECG interpretation has shown roughly double the sensitivity of STEMI criteria while maintaining comparable specificity [3].
The patients we miss do not have smaller infarcts just because the tracing does not meet STEMI criteria.
Khan’s meta-analysis of more than 40,000 NSTEMI patients found that about one in four had a totally occluded culprit artery, and that NSTEMI subgroup with total occlusion had substantially higher mortality than NSTEMI patients without total occlusion [4]! McLaren’s group later described the quality gap plainly: STEMI systems track false-positive activations, but often ignore the false negatives [5].
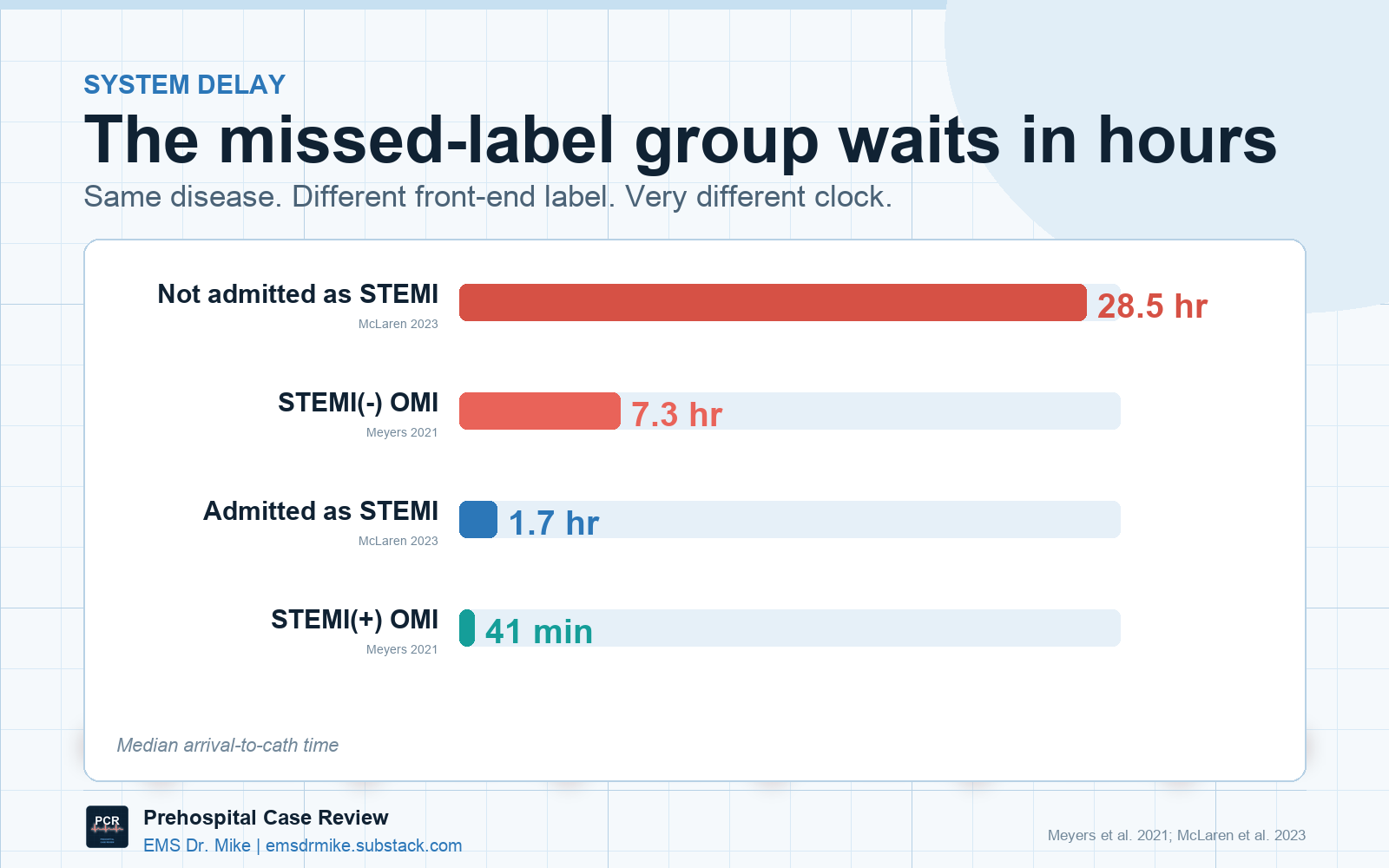
The delay is the part that should bother EMS clinicians … all acute care clinicians! In Meyers’ cohort, STEMI-positive OMI patients went to cath in a median of 41 minutes. STEMI-negative OMI patients waited 7 hours [2]. McLaren’s missed-occlusion cohort found door-to-cath times stretching past 28 hours for OMIs not admitted as STEMI [5]. A 2025 study focused specifically on acute total LAD occlusion found that 38% did not meet STEMI criteria on any pre-angiography ECG, despite similar infarct size and longer door-to-balloon times [6].
That delay is not only a cardiology problem. It is a systems problem. EMS sits at the front end of that system, and this is where high-risk ECG notification matters.
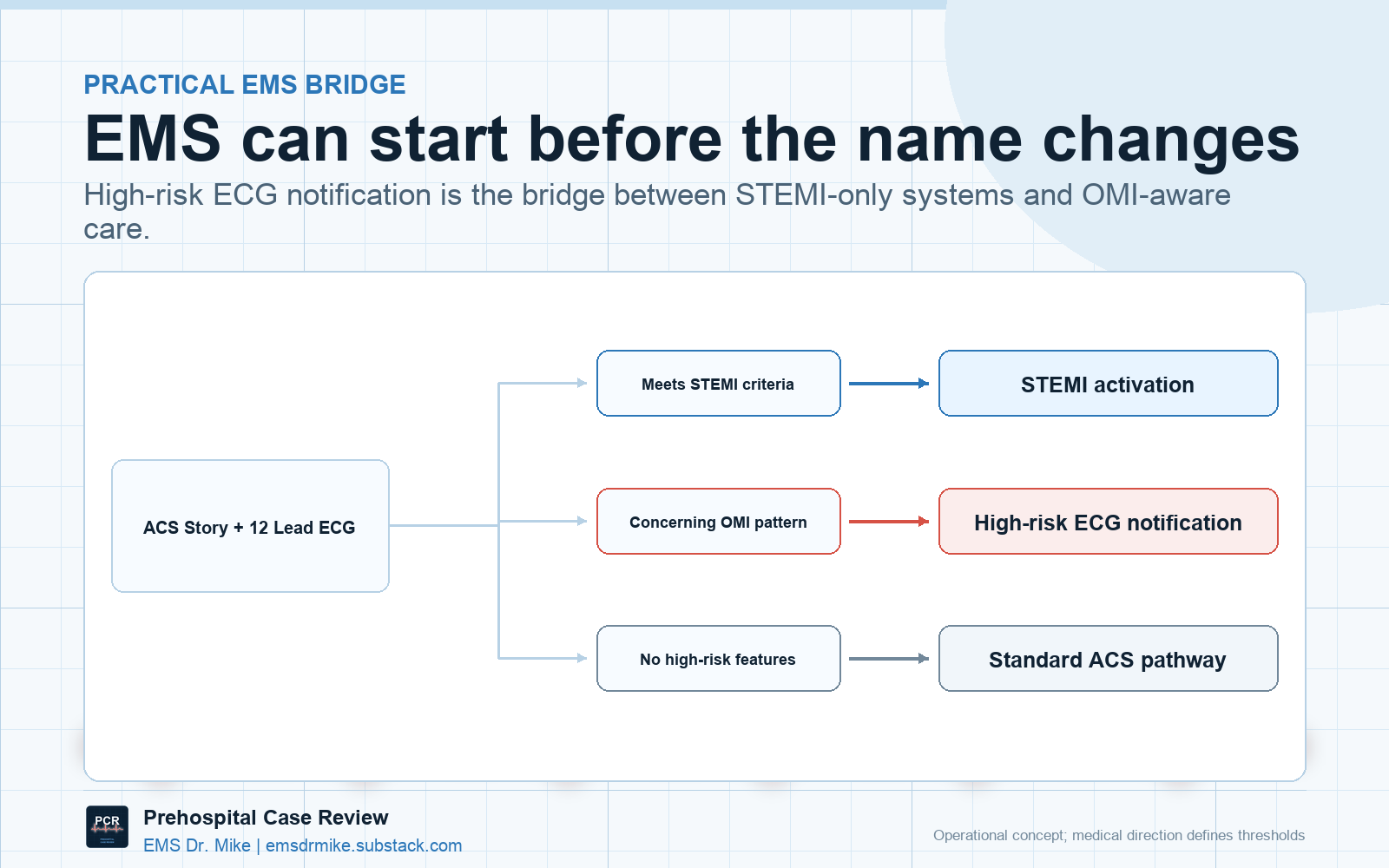
Not every system is ready for formal OMI activation. Most hospital systems are still built around STEMI activation, and that is not going to change because someone recognizes de Winter T waves at 2 a.m. But a system that is not ready for OMI activation still has room for a high-risk ECG notification.
The message is not, “We are activating your cath lab for a non-STEMI.” The message is, “We have a concerning clinical picture and a high-risk ECG. We are requesting the ED team meet us upon arrival.” That is a different request. It doesn’t activate the cath lab (…yet?), but it does tell the receiving team that this patient should not sit unseen behind three abdominal pains and a discharge-ready ankle sprain. The same pathway a high-functioning system takes for a prehospital patient arriving soon on BiPAP, or on pressors, or intubated - an expedited evaluation by the receiving ED team, with a warm handoff at bedside to the receiving clinicians.
The point is not to turn every chest pain into a cath lab alert; it is to give EMS clinicians a credible pathway for escalation when the tracing is more dangerous than the system’s interpretation.
OMI is where acute coronary care is headed.
The 2025 ACS guideline brought emergency medicine and EMS into the same combined ACS guideline space and continues to recognize high-risk ECG patterns, even though the formal system has not fully reorganized around OMI yet [9]. The Annals narrative review on OMI patterns makes the same conceptual move: ACS is not a disease defined by the ECG; the ECG is an imperfect test for an underlying pathology [10]. That distinction is going to become harder to ignore as the evidence keeps accumulating.
And the evidence is not the only thing changing. The technology is changing too.
AI-assisted ECG interpretation is going to be the force multiplier.
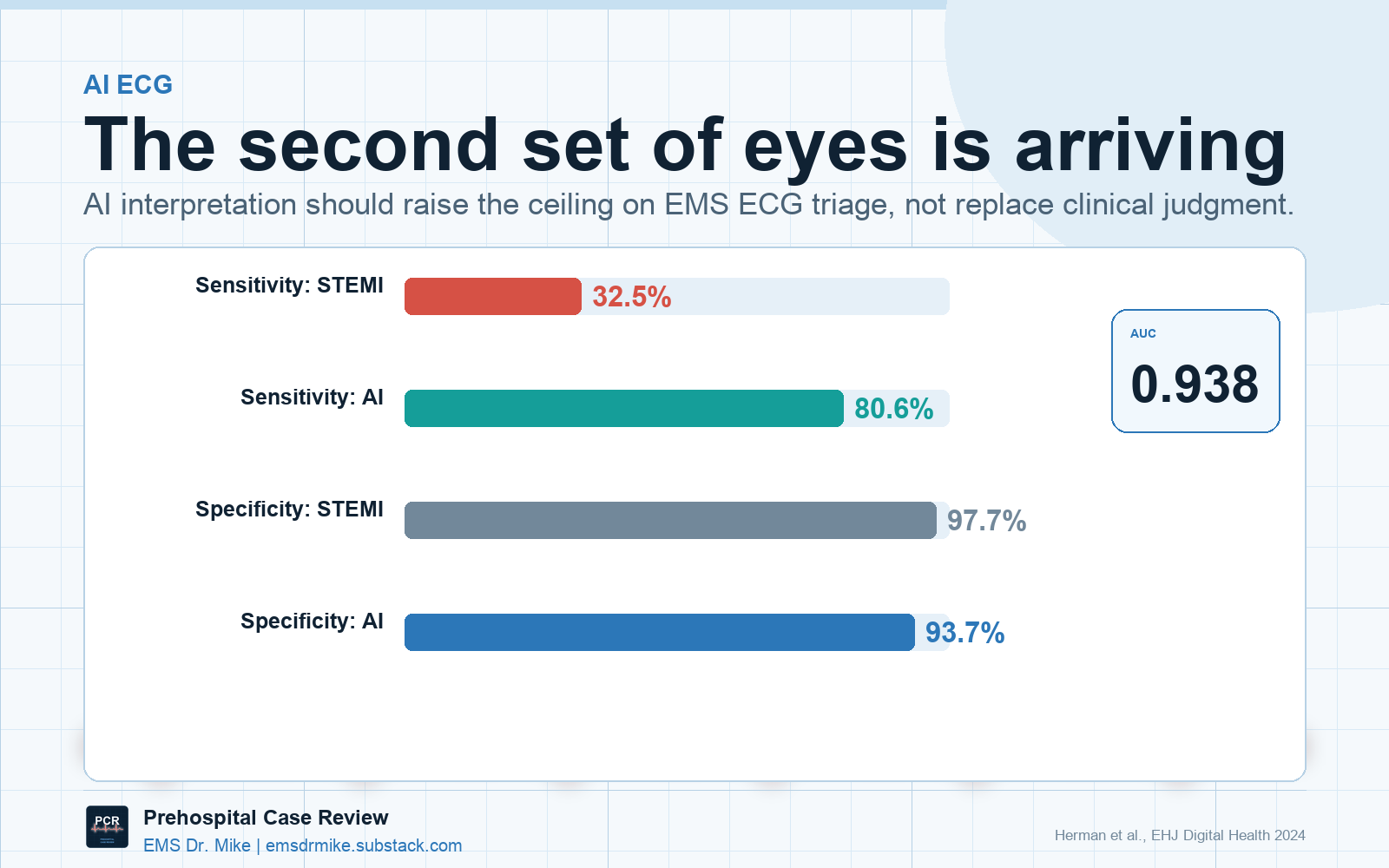
The Queen of Hearts model was trained to detect OMI using angiographic outcomes rather than STEMI labels. In an international validation dataset, it identified OMI with 80.6% sensitivity compared with 32.5% for conventional STEMI criteria, while keeping specificity high at 93.7% [7]. In the 2025 total LAD occlusion analysis, both expert interpretation and the AI model identified every STEMI-negative LAD occlusion on the first ECG in that dataset [6].
That signal has continued into real-world pathway work. A 2026 retrospective OMI Alert cohort found that Queen of Hearts identified 81% of angiographically confirmed OMIs overall and 66% of STEMI-negative OMIs using a high-confidence threshold [8]. And as that threshold keeps evolving, the important point for EMS is the trajectory: algorithms trained on occlusion are starting to support pathways that traditional STEMI labels cannot.
That is not a reason to hand the ECG to a black box and stop thinking. They are a reason to prepare EMS systems for a different kind of ECG support. The prehospitalist still has to meet the patient, obtain a clean tracing, repeat it when the story changes, recognize when the clinical picture does not fit the machine interpretation, choose a destination, and make the notification. AI does not replace that. It gives the field clinician a second set of eyes that has been trained on occlusion rather than on a single ST-segment threshold.
The endpoint is an OMI notification pathway.
High-risk ECG notification is the bridge until the rest of the system catches up. It gives EMS a way to act on the future of acute coronary care without pretending every hospital has already adopted it. It also gives medical directors a practical place to start: define the patterns, write the notification language, train crews on OMI and serial ECG acquisition, and build a Just Culture-based QA loop that reviews these cases for learning rather than blame.
There will be false positives, as there are in STEMI activation now. The answer to that is measurement: track which high-risk ECG notifications went to cath. Track which did not. Track missed occlusions. Track whether the notification changed time to physician review, repeat ECG, cardiology consultation, or cath. EMS has spent years proving that prehospital activation can move time-sensitive systems. OMI is the next version of that work, and part of that system design impetus rests upon us.
We should keep calling STEMIs when the tracing meets criteria. That pathway saves lives and does not need to be torn down. But we also need to stop acting as though a patient is lower risk simply because the ECG did not satisfy a threshold designed for an earlier era. An occluded artery is still an occluded artery. If the field clinician sees the risk, the system needs a way to hear it.
The evidence increasingly suggests that we are missing occlusions and delaying reperfusion for patients who never met STEMI criteria. EMS helped build modern STEMI systems. We should help build what comes next.
Thanks for reading! Subscribe for free to receive new posts and support my work. Free open access medical education for EMS clinicians by EMS physicians.
References
de Alencar Neto JN, Scheffer MK, Correia BP, Franchini KG, Felicioni SP, De Marchi MFN. Systematic review and meta-analysis of diagnostic test accuracy of ST-segment elevation for acute coronary occlusion. Int J Cardiol. 2024;402:131889. doi:10.1016/j.ijcard.2024.131889.
Meyers HP, Bracey A, Lee D, Lichtenheld A, Li WJ, Singer DD, et al. Comparison of the ST-elevation myocardial infarction versus NSTEMI and occlusion MI versus NOMI paradigms of acute MI. J Emerg Med. 2021;60(3):273-84. doi:10.1016/j.jemermed.2020.10.026.
Pendell Meyers H, Bracey A, Lee D, et al. Accuracy of OMI ECG findings versus STEMI criteria for diagnosis of acute coronary occlusion myocardial infarction. Int J Cardiol Heart Vasc. 2021;33:100767. doi:10.1016/j.ijcha.2021.100767.
Khan AR, Golwala H, Tripathi A, Bin Abdulhak AA, Bavishi C, Riaz H, et al. Impact of total occlusion of culprit artery in acute non-ST elevation myocardial infarction: a systematic review and meta-analysis. Eur Heart J. 2017;38(41):3082-9. doi:10.1093/eurheartj/ehx418.
McLaren JTT, El-Baba M, Sivashanmugathas V, Meyers HP, Smith SW, Chartier LB. Missing occlusions: Quality gaps for ED patients with occlusion MI. Am J Emerg Med. 2023;73:47-54. doi:10.1016/j.ajem.2023.08.022.
Meyers HP, Sharkey SW, Herman R, de Alencar JN, Shroff GR, Frick WH, et al. Failure of standard contemporary ST-elevation myocardial infarction electrocardiogram criteria to reliably identify acute occlusion of the left anterior descending coronary artery. Eur Heart J Acute Cardiovasc Care. 2025;14(7):403-11. doi:10.1093/ehjacc/zuaf037.
Herman R, Meyers HP, Smith SW, et al. International evaluation of an artificial intelligence-powered electrocardiogram model detecting acute coronary occlusion myocardial infarction. Eur Heart J Digit Health. 2024;5(2):123-33. doi:10.1093/ehjdh/ztad074.
Hellerman MB, Wang C, Zhang DT, Kalogeropoulos AP, Skopicki HA. Detecting occlusion myocardial infarction with an AI-powered ECG model: a retrospective cohort study. J Pers Med. 2026;16(4):174. doi:10.3390/jpm16040174.
Rao SV, O’Donoghue ML, Ruel M, Rab T, Tamis-Holland JE, Alexander JH, et al. 2025 ACC/AHA/ACEP/NAEMSP/SCAI guideline for the management of patients with acute coronary syndromes. J Am Coll Cardiol. 2025;85(22):2135-2237. doi:10.1016/j.jacc.2024.11.009.
Ricci F, Martini C, Scordo DM, et al. ECG patterns of occlusion myocardial infarction: a narrative review. Ann Emerg Med. 2025;85(4):330-40. doi:10.1016/j.annemergmed.2024.11.019. == Title is Beyond STEMI in EMS: Why EMS Needs a High-Risk ECG Notification Pathway
AI interpretation of a 12 lead sounds like a reliable tool, but when I ask AI questions there’s always a note that says AI is fallible and to double check important information. I’m not sure which AI was used in the study you referenced, AI can be reliable at certain things, and it seems like 12 lead interpretation is an excellent use that could save lives and reduce long term repercussions for patients.
Do the new monitors that are coming out have AI embedded in the 12 lead part of their magic? Now I’m wondering how the lifepak or zoll comes up with it’s interpretation, that will be my next rabbit hole to disappear down, lol.
I’ve done a lot of 12 leads and don’t rely on the monitor’s interpretation very often because it’ll call something a STEMI that is definitely not a STEMI and it’ll call a 12 lead that is a STEMI something else. I’m also old, started in EMS when all we had were LP5’s and the smell of burning paper when it jammed. I may or may not have set a pt’s chest hair on fire by having the manual paddles a little too close together.
Thank you for sharing this, AI is definitely changing almost everything in our world, and this could spare me having to go toe-to-toe with a charge nurse when my pt’s LLS score is high but the 12 lead is unconcerning.
Great post!
I have adopted the phrase "this EKG does not meed STEMI criteria however, due to (winters waves, Wellen's patterns, Sgarbossa etc..) I am concerned that have ongoing myocardial ischemia. We're coming in light and sirens".
It's an end-run around formal STEMI criteria towards the OMI/NOMI paradigm. Whether it gets me an activated cath lab team is VERY doc or hospital dependent but it works more than you'd think. At least here in Denver.